Orthopedic Care for Locking Finger Symptoms in Wellington, Florida
Trigger finger, also called stenosing tenosynovitis, affects the tendons that bend the fingers and thumb. AAOS explains that these flexor tendons travel through tendon sheaths as they move from the forearm across the palm and into each digit. Along the way, tissue bands called pulleys hold the tendons close to the bones so the fingers can bend efficiently.
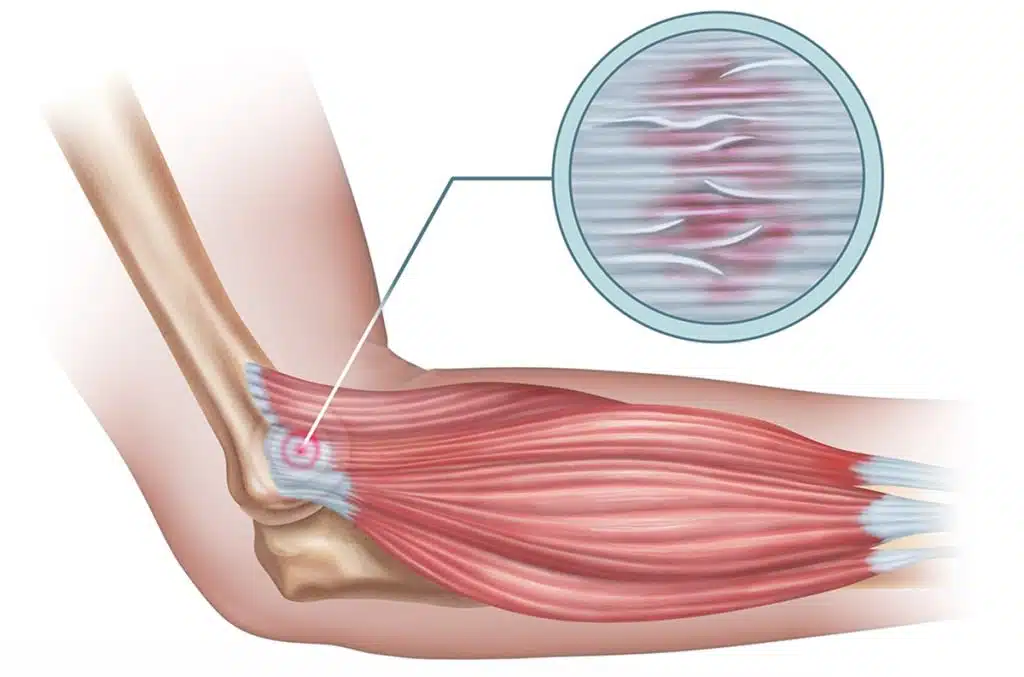
The pulley most often involved is the A1 pulley at the base of the digit where it meets the palm. AAOS notes that in trigger finger, this pulley becomes thickened and inflamed, making it harder for the tendon to glide through normally. Over time, the tendon itself may also become irritated and develop a small nodule. When that thickened tendon tries to pass through a tightened pulley, the result is catching, popping, pain, or locking.
The Orthobullets episode frames trigger finger as a high-yield hand condition, which makes sense because the mechanics are straightforward but the daily impact is big. A very small space problem can create a very noticeable function problem.
Why trigger finger feels so strange to patients
A lot of musculoskeletal issues cause pain, but trigger finger often adds something that feels unsettling. The digit does not just hurt. It behaves unpredictably. One moment it moves normally. The next it clicks, sticks, or locks in a bent position.
AAOS describes common symptoms such as:
- a tender lump at the base of the finger or thumb on the palm side
- a catching, popping, or locking sensation with movement
- pain when bending or straightening the digit
- morning stiffness or worse symptoms after inactivity
- a digit that may become stuck in a bent position in severe cases
This is why patients often say the hand feels unreliable, not just painful. They may avoid gripping because they are waiting for the next painful pop. They may use the other hand to open the finger. They may change how they hold objects without even realizing it.
Which fingers are usually affected
AAOS notes that the ring finger and thumb are the most commonly affected digits, though trigger finger can involve any finger. When the thumb is involved, it is often called trigger thumb.
That matters because the impact can look a little different depending on the digit involved. A thumb that catches may interfere with pinching, opening containers, typing, texting, writing, and holding utensils. A ring finger or middle finger that locks may affect grip strength, lifting, weight training, golf, gardening, and repetitive tool use.
In Wellington, the patient may be a parent lifting gear, an office worker typing all day, a golfer gripping clubs, a fitness enthusiast using dumbbells, an equestrian managing reins and tack, or someone doing repetitive chores and meal prep. Hand problems rarely stay isolated to one tiny task.