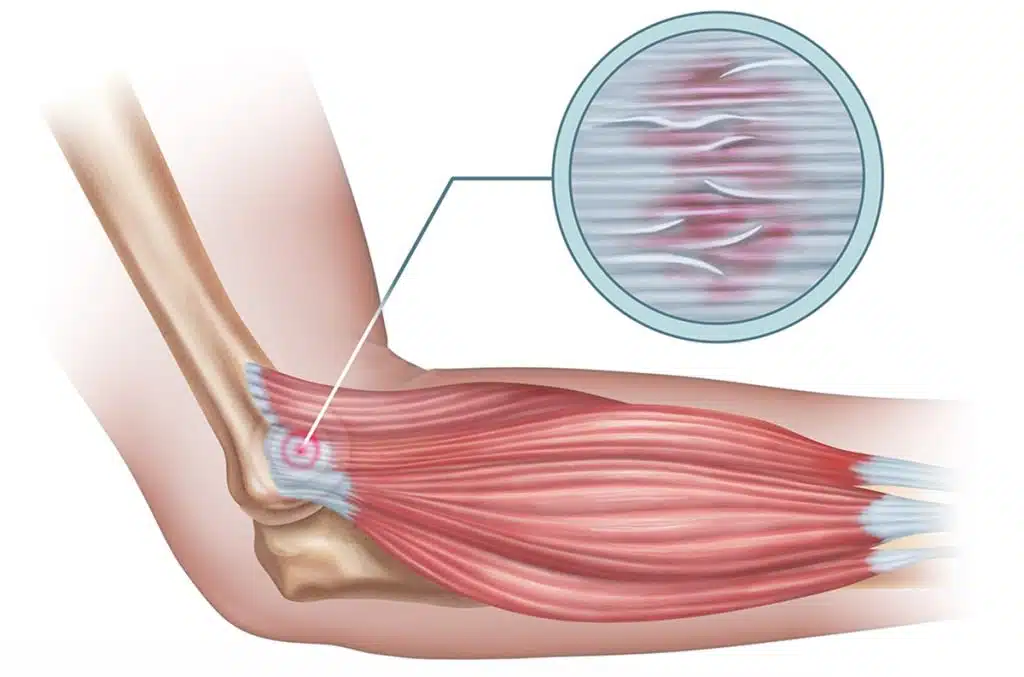
Golfer’s elbow is also called medial epicondylitis. AAOS explains that it affects the tendons of the forearm muscles that attach to the inside of the elbow at the medial epicondyle. These muscles help rotate the forearm inward and flex the wrist and fingers, which means they are involved in more daily activity than most people realize.
The AAOS review notes that one of the most commonly affected muscles is the pronator teres, although several tendons in the same region can be involved. That helps explain why symptoms can feel diffuse at times. One patient points to one sharp spot near the inner elbow. Another feels pain spreading toward the forearm when gripping, lifting, or twisting. Someone else mainly notices weakness and reduced confidence in the arm.
The podcast source makes the condition easy to picture in real life. If every time you grip tightly or turn the palm downward you keep pulling on the same irritated tendon attachment, the tissue never really gets a chance to settle. In Sebring, that can happen during golf, racquet sports, weight training, repetitive household chores, mechanical work, landscaping, warehouse lifting, or ordinary daily routines that keep loading the same structures.
Why the name golfer’s elbow can be misleading
A lot of patients hesitate to take the diagnosis seriously because they think, I do not even play golf. But AAOS is clear that many activities can cause medial epicondylitis, including overhead throwing, tennis, weightlifting, repetitive daily tasks, and non-sport activities with no single obvious injury.
That is important because people who do not identify with the label golfer’s elbow often keep brushing symptoms off. They assume it is just a minor strain or that it will settle if they ignore it for a week or two. Sometimes it does ease briefly. But if the same tendon keeps getting loaded by the same tasks, symptoms often come right back.
The real issue is not whether you swing a club. It is whether the tissues on the inside of the elbow are being stressed faster than they can recover.