What PRP Is Not
PRP is not magic. It is not an instant numbing shot. It is not a guaranteed way to rebuild a damaged tendon. It is not automatically superior to rehabilitation, activity modification, or careful load management. It is also not a substitute for a correct diagnosis.
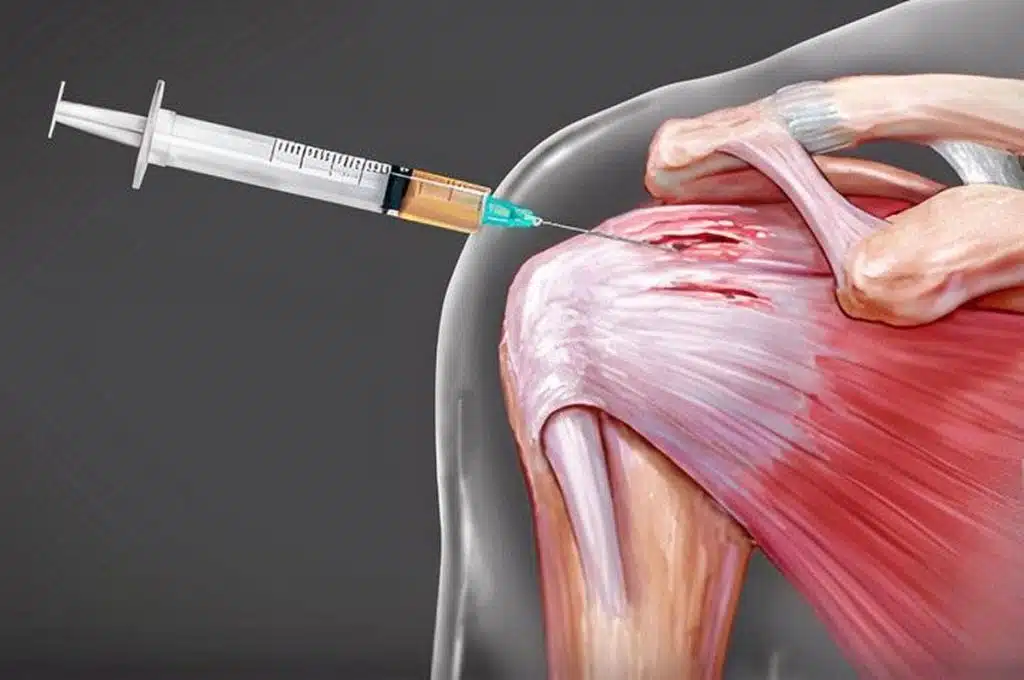
This matters because shoulder pain has many possible sources. Rotator cuff tendinopathy is common, but pain can also come from adhesive capsulitis, shoulder arthritis, biceps tendon irritation, labral problems, cervical nerve irritation, instability, calcific tendinitis, or referred pain. If the diagnosis is wrong, even a technically perfect PRP injection may disappoint.
A responsible regenerative orthopedic plan should start with a careful history, physical exam, and appropriate imaging. The clinician should identify the most likely pain generator, explain why PRP may or may not fit, and discuss alternatives. The best doctors do not sell PRP to every patient. They select it when the patient’s problem, goals, and tissue status make the option reasonable.
Who May Be a Good Candidate
A patient with persistent rotator cuff tendinopathy may be a reasonable PRP candidate if symptoms have not improved enough with conservative care, the tendon is painful but not clearly beyond repair, and the patient wants a non-surgical option with realistic expectations. This may include someone who cannot sleep on the affected side, struggles with overhead activity, has pain during exercise, or wants to avoid repeated steroid injections.
The best candidate is usually willing to participate in the recovery plan. PRP may help the tendon environment, but the shoulder still needs appropriate loading. That means a staged return to strength, mobility, and activity. If the shoulder keeps being overloaded immediately after the injection, results may suffer. If the patient avoids all movement for too long, stiffness and weakness may become bigger problems.
Patients with a full-thickness traumatic tear, major weakness, severe arthritis, advanced stiffness, or nerve symptoms may need a different approach. PRP might still be discussed in selected cases, but it should not delay necessary care when surgery, targeted rehabilitation, or another diagnosis is more appropriate.